Atrial Fibrillation Patient Guide: What You Need to Know
Learn all the essential facts of atrial fibrillation for yourself or a loved one.
Andrew Hinojos, DO
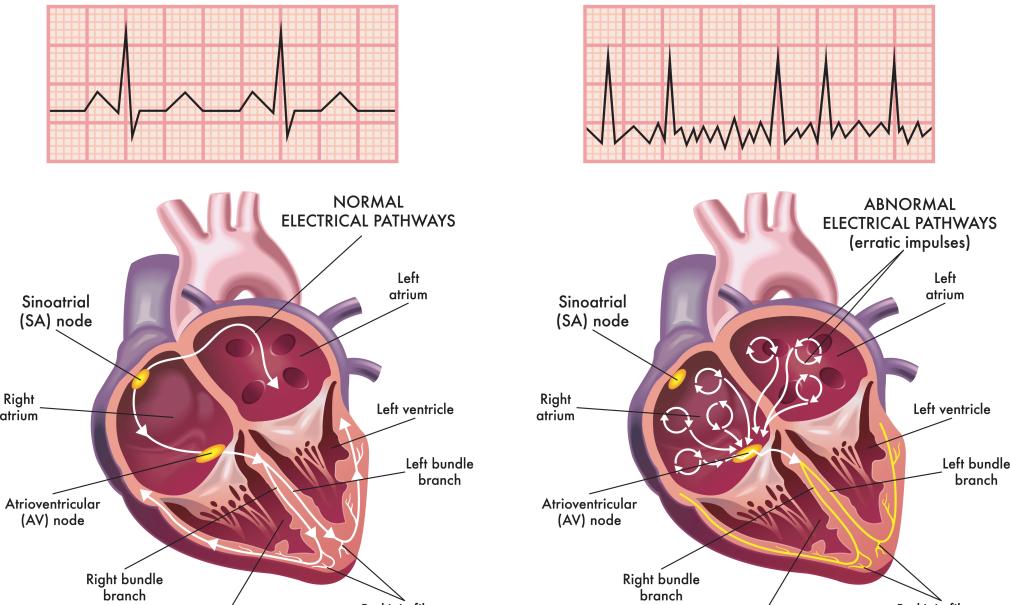
Atrial fibrillation (AF) occurs when the upper chambers of the heart (atria) beat rapidly and in an uncoordinated manner (fibrillation). This uncoordinated, rapid beating affects the flow of blood through the heart, causing an irregular pulse.
AF is the most common type of heart rhythm disorder. The risk of developing it significantly increases with age; about 1 in 10 people over the age of 70 have AF. While AF is manageable, it can progress to the point of causing a stroke if untreated.
I’m Dr. Andrew Hinojos with the Saint Francis Heart and Vascular Institute, and in this article I’ll outline everything you need to know about recognizing, treating and managing AF for you and your loved ones.
What are the symptoms?
During an episode of AF, the most common symptoms are:
- heart palpitations (irregular or rapid heartbeat)
- irregular pulse
- shortness of breath
- weakness
- fatigue
- dizziness or light-headedness
- exertional intolerance (exhaustion/shortness of breath from walking short distance, climbing a few stairs, etc.)
Some people may experience worsening symptoms of congestive heart failure such as fluid accumulation in the lungs or extremities (edema).
Symptoms tend to be non-specific and sometimes people may experience minor or no symptoms at all.
How is AF diagnosed?
While feeling an abnormal or irregular pulse may suggest AF, the only true way to diagnose it is to record the irregular heart rhythm.
This can be done with an electrocardiogram (EKG) or a heart monitor worn for an extended period.
What causes AF?
Normally, the four chambers of the heart beat in a synchronized, controlled manner to circulate blood from the heart to the lungs, back to the heart and then to the rest of the body.
The heartbeat is controlled by specialized areas of heart tissue that act as the heart’s pacemaker (called the sinus node and atrioventricular or AV node). These areas control electrical impulses through the heart muscle and ensure regular, coordinated muscle contractions.
Triggers or electrical firing from the pulmonary veins in the left upper chamber (atrium) can fire and put someone’s heart into AF.
Are there different types of AF?
Yes, AF is classified according to how frequently the episodes occur and how quickly they go away. It is further classified as:
- Paroxysmal atrial fibrillation - AF that is intermittent and stops within 7 days of onset. Often the heartbeat spontaneously “converts” back to normal rhythm.
- Persistent atrial fibrillation - AF that is continuous and sustains for >7 days. This type requires intervention to restore the heart back to normal rhythm. It is typically considered a progressed stage of AF.
- Long-standing persistent atrial fibrillation - AF that is continuous for >12 months.
- Permanent atrial fibrillation – This describes a heart that is always in AF and the patient and health provider have mutually decided not to make any further attempts at restoring normal rhythm.
What are the risks associated with AF?
AF is typically a chronic condition and there is no cure. It commonly, but not always, progresses over time to higher burdens and becomes more sustained.
Stroke is the greatest risk associated with AF.
When the heart is in AF, blood is not always pumped completely out of the atrium. If the blood is not flowing correctly, a blood clot could form in the atrium. The clot may travel to an artery supplying blood to the brain and cause a blockage (a stroke).
The focus of treatment is to prevent stroke and manage symptoms, with an initial focus on evaluating and minimizing the overall burden of AF.
What are ways to prevent stroke from AF?
Not everyone that has AF has the same risk of stroke. For those at higher risk, anticoagulant medication is the standard intervention. For those who have bleeding risks, inserting an occlusion device into the left atrial appendage (a small finger-like projection from the heart’s upper left chamber) may be considered.
Your provider will review your individual risk factors and make recommendations on whether a blood thinner (anticoagulant) would be appropriate to reduce the risk of blood clotting and stroke.
Because the left atrial appendage is where clots are most likely to form, there are left atrial appendage closure devices that can seal this area off and prevent AF blood clots. Patients will require a blood thinner to prevent blood clots from forming on the device as tissue grows over it.
There is also a risk of blood clots forming in other areas of the top chambers of the heart when in AF. Because of this potential complication, occlusion devices are typically reserved for individuals that cannot stay on blood thinners long term.
It is important to note that these devices do not treat atrial fibrillation and only help reduce the risk of stroke in patients with increased bleeding risk when someone is in AF.
What are the treatments for atrial fibrillation?
Treatment will vary depending on the type of AF you have and how it affects you. In terms of rhythm control treatment for atrial fibrillation, these are the following options:
- Anti-arrhythmic drug therapy
- Catheter ablation
Your provider will discuss the options for treatment and will discuss specific recommendations for you based upon the type of AF and how it affects you.
What is catheter ablation?
Catheter ablation is a minimally invasive, outpatient procedure in which flexible wires (catheters) are inserted into the heart through a blood vessel in the groin. The catheter is then used to destroy the small areas of heart tissue generating the abnormal electrical activity that causes AF.
Catheter ablation is not curative of AF but does help 70-80 percent of patients maintain normal sinus rhythm depending on their AF classification. In general, patients with AF who have had catheter ablation have significantly fewer episodes that are shorter in duration and less symptomatic.
Catheter ablation has been shown to prevent the progression of persistent atrial fibrillation from paroxysmal atrial fibrillation compared to antiarrhythmic drug therapy. In patients with reduced heart function or congestive heart failure, catheter ablation has been shown to significantly reduce the risk of cardiovascular death or hospitalization for heart failure compared to medical therapy.
What medications are available for AF?
Medications like beta blockers or calcium channel blockers may be prescribed to reduce the frequency of and/or to control the rapid heartbeat.
Other rhythm control medications (reduce frequency of rapid heartbeat) include:
- Sotalol
- Flecainide
- Propafenone
- Dofetilide
- Dronedarone
- Amiodarone
These anti-arrhythmic medications are designed to help reduce the frequency of symptomatic atrial fibrillation episodes. Your provider will review which medication may be appropriate for you based upon your health profile.
What is a cardioversion?
A cardioversion is a simple procedure that uses an electric shock to reset the heart and restore normal sinus rhythm. This is simply a reset of the heart’s electrical conduction system; it does not prevent future episodes of AF.
How can I lower my risk for atrial fibrillation?
Lose weight and maintain a healthy weight: Weight loss is a powerful tool that significantly impacts AF. Reducing 10 percent of overall body weight has been proven to reduce AF symptoms, burden, recurrence, and progression. If necessary, we may refer you to Lifestyle Medicine to assist you in achieving a healthy weight.
Exercise regularly: Moderate-to-vigorous exercise approximately 3.5 hours per week is recommended to reduce AF symptoms and burden, increase maintenance of sinus rhythm, increase functional capacity, and improve overall quality of life.
Treat sleep apnea: If you have been diagnosed with sleep apnea, it is very important that you use your sleep device as prescribed by your sleep specialist.
If you have not been diagnosed with sleep apnea but have symptoms (as determined by your health care provider) have a sleep study to get a diagnosis and proper treatment for it. Although sleep apnea is not considered a cause of AF, treated sleep apnea helps prevent recurrence and progression of AF.
Minimize or eliminate alcohol consumption: Men should have no more than 2 drinks per day and women no more than one drink per day. Some patients are sensitive to even the smallest amounts of alcohol, so they should avoid alcohol as a direct aggravator of their AF.
Stop smoking: If you use tobacco products, we strongly encourage you to stop. We have resources to help you quit.
Control blood pressure: Optimal BP control is recommended to reduce AF recurrence and AF-related cardiovascular events. Take blood pressure medications as prescribed by your health provider.
Get essential heart screenings at a reduced rate: Prevention & Screenings
Learn more about Saint Francis Heart and Vascular Institute: HVI Home page




